
Gore/Paquette Oral Boards
Case 1. Adult male stabbed in the left chest. Chest tube is placed and patient was intubated. Patient becomes pulseless. ED thoracotomy was performed. Patient was found to have a tense pericardium when the chest was opened. Incising the pericardium released blood and the patient’s pulses returned. Diagnosis was pericardial tamponade from a stab wound to the heart. Once the pericardial sac is opened and the tamponade is released vital signs will often return. The wound can be stapled or occluded with a finger or foley balloon. The patient was transported up to surgery.
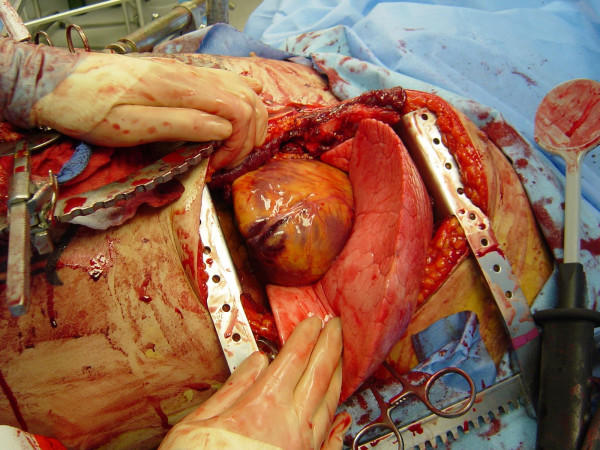
*ED thoracotomy
Elise comment: Male patients who need emergent blood transfusion can receive O positive blood. Only women need O negative blood.
Girzadas comment: Stab wounds to the chest are the most likely injury in which an ED thoracotomy can save a patient’s life. These type of injuries can have tamponade without extensive myocardial injury. If the thoracotomy is done rapidly these patients can survive.
Case 2. 55yo male with severe left flank pain. BP=100/50, P=140. Patient has history of smoking and HTN. Bedside U/S shows:

*Bedside U/S
Diagnosis was ruptured abdominal aortic aneurysm. Patient was transferred to surgery emergently.
Teaching point: If a patient with the history of hypertension develops hypotension you know there is a significant problem.
Case 3. 3 yo male with seizure and lethargy. Blood sugar was 10. History revealed that there was a Christmas party at the home the previous night and the child had ingested left-over ETOH. The patient’s ETOH level was 180. Urine toxicology screen was negative. Critical actions were to correct the blood sugar with dextrose.
Bill Schroeder’s Rule of 50
Age less than one month: 5ml/kg of D10 (5 x 10=50)
Age one month to 2 yrs: 2 ml/kg of D25 (2 X 25=50)
Age over 2 years: 1 ml/kg of D50 (1 X 50= 50)
This patient would receive 1ml/kg of D50 to correct blood sugar.
Also have the crisis worker discuss with patient and consider notifying DCFS for child endangerment.
Iannitelli Wound Ballistics and ED Management of Gun Shot Wounds
Guest Speaker Darin Crowder US Army Retired Master Sergeant
Case: 30yo male with small caliber/low velocity GSW to left low back. Patient is alert and talking but BP is 100/50 and heart rate is 130. Patient has no respiratory distress. Hypotension improved with IV fluid bolus. While getting a chest xray, patient becomes bradycardic. Chest xray shows hemothorax on right and bullet in the right chest. Patient arrests soon after chest xray. CPR started, patient was intubated and a right chest tube was placed. Epinepherine given. Patient had ROSC Patient made it to OR where he was found to have an IVC/RA junction injury.
Extent of patient injury depends on how much kinetic energy is transferred from the bullet to the tissue.
Shotguns have an effective range of 25 yards. It is intended to be used to kill birds. It is an “area” weapon. Shotgun pellets spread out in a cone fashion across the target area. There are 300 pellets in a shotgun shell. The wadding in a shotgun shell can cause injury up to 5-10 yards.
Rifles have a range from 50-6000 yards. It is designed to be accurate and lethal over long ranges.
Handguns have a maximum effective range of around 25 yards.
Maximum effective range does not equal lethality. Maximum effective range is the range that the shooter can expect to accurately hit a target. A bullet from a handgun can travel up to a mile and even kill someone at that distance, but the shooter can’t effectively control the trajectory of the bullet for a mile.
Caliber is the diameter of the projectile. 30 caliber is a projectile with a 0.3 inch diameter. 9mm=38caliber=.38inches diameter
There is rifling (grooves) in the barrel of a rifle that causes the bullet to spin which increases the accuracy of the bullet. Pistols have less rifling in the barrel so there is less accuracy. With less spin, the bullet will develop yaw (tilt off of the path of the trajectory) which throws off the accuracy.
Small caliber bullets have a higher initial muzzle velocity than higher caliber bullets.
Smaller caliber bullets have less powder in the casing. There is less recoil with small caliber bullets. Shooters generally prefer smaller caliber bullets so that it is less painful to shoot due to less recoil.
Handguns are typically high velocity(>1100ft/s) rounds.
Jacketed and non-jacketed bullets: Jacketed rounds have a lead core with a metallic shell so that the bullet will maintain its integrity as it passes through a target. Non-jacketed rounds don’t have a metallic covering so the bullet deforms and transfers all its energy into the target.
Hollow point bullets are meant to break apart and deform on contact in order to transfer as much energy into the targeted person. This is called stopping power. It is intended to stop a person with a single bullet.
Damage to the patient depends on how much kinetic energy is transferred from the bullet to the patient.
- Kinetic energy of the bullet at impact is its maximum capacity for injury. 1/2mv2 =kinetic energy
- Kinetic energy doesn’t equal energy transferred. Energy transferred to the target is proportional to low speed (like getting stabbed with a spoon vs. a knife. If they both penetrate the body the spoon is going to do more damage). Energy transfer is also greater with yaw, bullet deformity, and larger caliber projectile.
- Yaw is when the bullet tilts or tumbles off the direct path it is travelling.
- Permanent cavitation is the damage done by the bullet projectile (crushing/tearing)
- Temporary cavitation is the lateral displacement of tissue around the projectile as it passes through the body. Tissue stretches around the path of the bullet. This causes much tissue damage.

*Yaw and Tumble
Bystanders that are struck by bullets at a distance out of the effective range of a handgun can suffer significant injury because at these distances there is a lot of yaw and tumbling occurring. Thus the bullet hits at a lower speed with yaw and this usually results in a lot of energy transfer to the victim.
Girzadas question: If low velocity rounds transfer more energy to a targeted victim, why do military weapons use high velocity rounds. Darin’s reply: Milatary weapons/rounds are intended to engage the enemy at a longer distance. To get accurate shots at longer distances you need higher velocity rounds. The military has found that in close quarter fighting, high velocity rounds pass through the victim without stopping them (without much energy transfer). The military has switched to lower velocity/higher caliber weapons/ammunition for close quarter fighting to stop enemy combatants more effectively. These low velocity, high caliber rounds impart more energy into the target and have more stopping power.
Doherty comment: It is difficult for front line treating physicians to know whether a gun shot wound is an entry or exit wound. He advised not making that determination in the medical record because you may have to testify against a forensic pathologist.
In retrospect, the chest xray had some very telling clues. The bullet had traversed the body from left to right (transmediastinal) and definitely had undergone significant yaw (The bullet was tilted and pointed out of the direction of the bullet path). The bullet had not deformed so it was jacketed. Thus the bullet had transferred significant energy to the patient based on yaw and it’s pathway put vital mediastinal structures at risk.
Doherty comments: The initial chest xray is a key indicator to where the surgeon should approach the operative repair of gunshot wound injuries.
When looking at xrays the number of wounds plus bullets should be an even number. If it is not then you need to find another bullet.
Htet Safety Lecture
85 yo female with atrial fibrillation on warfarin. Patient presented with abdominal pain. Patient was sent to CT scan for imaging. In the CT scanner she fell and hit her head. She suffered a subdural hemorrhage. Patient was managed with FEIBA and neurosurgery consultation.
Natalie discussed the Michigan Model of risk reduction which features admitting a mistake occurred, quick settlement, and an apology. This has been shown to reduce the number and cost of claims.
At ACMC, all reported safety events are reviewed/vetted by a patient safety officer and the PI committee. A Root Cause Analysis is done if needed.
Elise comment: Is Advocate moving toward the Michigan model? Htet response: yes, we still have a way to go but the safety team and risk management are working on it.
To avoid patient falls in the ED:
- High risk patients are identified
- Yellow fall-risk wrist bands are applied.
- Non-skid socks are used
- Patients are assisted to the bathroom
Research has not been able to identify a single risk factor to predict a fall in the next 6 months. Relative factors related to falls that were identified were depression, foot sores, limited functional mobility, and previous falls.
Lambert U/S GB, Kidneys, Abdominal Aorta
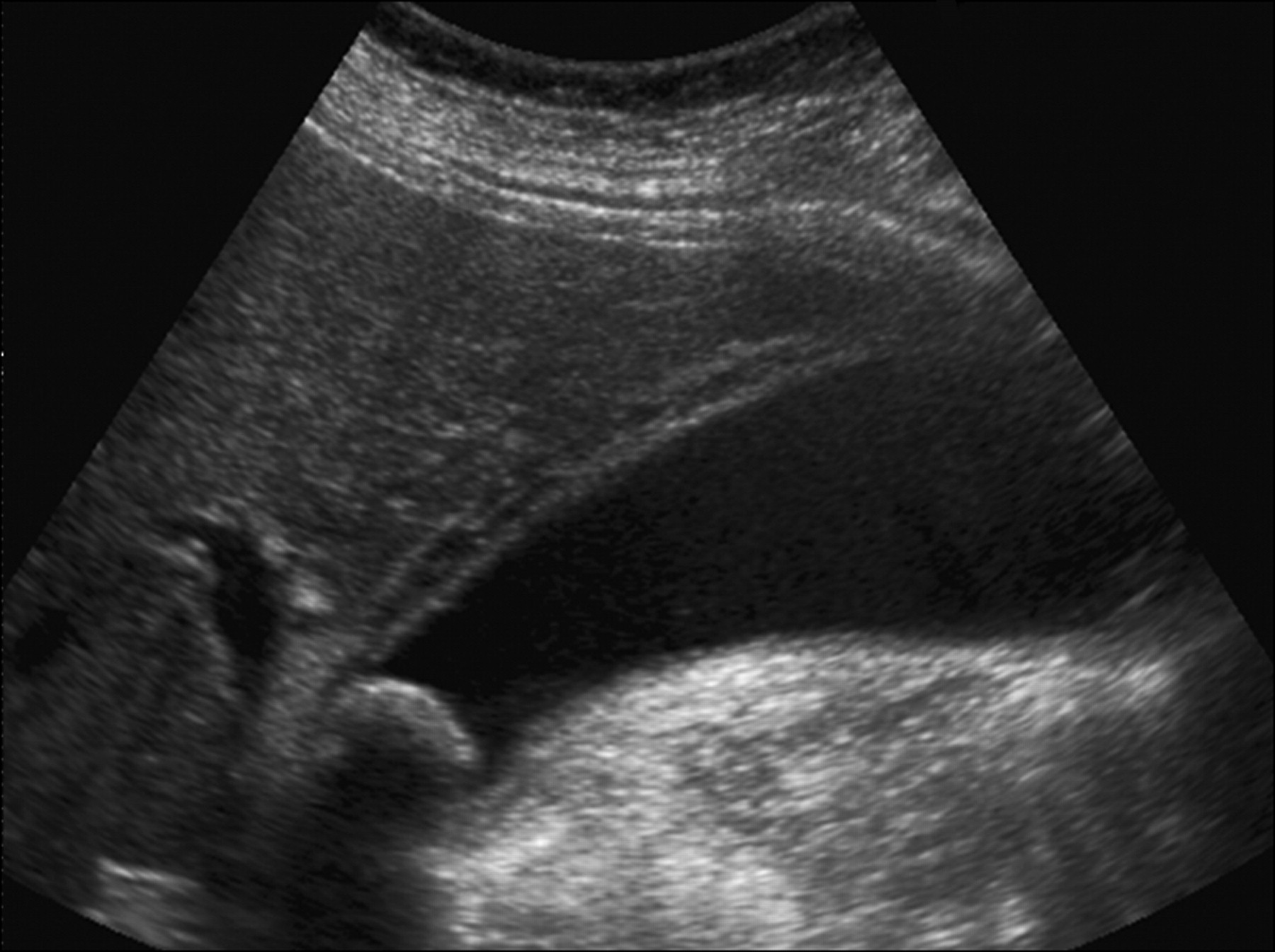
A nice window to image the gallbladder is through right ribs. The more traditional window is X -10 or 10cm to the right of the xyphoid.
You want to see the main lobar fissure with the GB in the longitudinal plane.
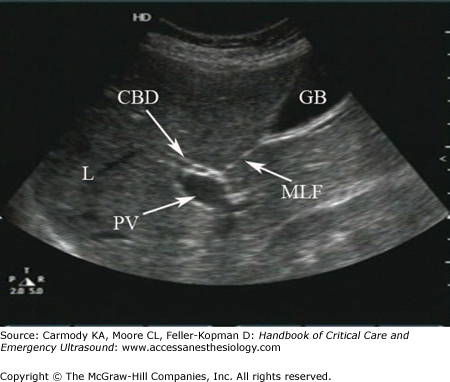
*Longitudinal view of GB with main lobar fissure seen.

*Gallstones with shadowing

*Wall echo shadow The stones in the gall bladder are close to the anterior wall and shadowing is obscuring the entire gall bladder.
*GB wall thickening is 4mm or more at the anterior wall. There is also pericholecystic fluid. A gallstone also imaged.
*Hydronephosis grading

*Seagull Sign Celiac Trunk which is the first branch off the abdominal aorta. Celiac trunk splints into the splenic artery and hepatic artery.
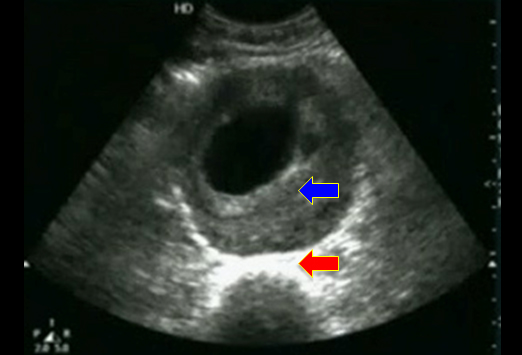
*Abdominal Aortic aneursysm. Blue arrow is pointing to aneurysm and clot. Red arrow is pointing to anterior border of spine.
If you see an older patient with groin pain you should also image the iliac arteries. Mike has seen 3 iliac artery aneurysms in octogenarians. If you just image down to the bifurcation of the aorta you may miss the iliac artery aneurysm.
U/S Workshop
