Remke/E. Kulstad Oral Boards
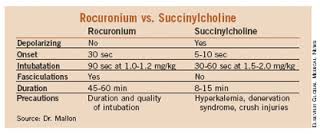
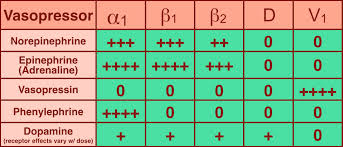
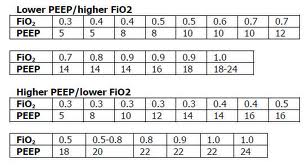
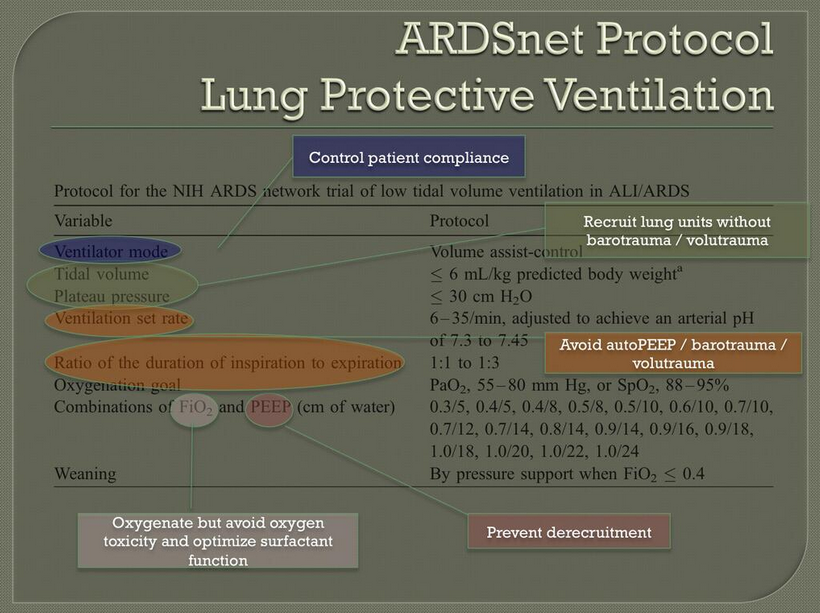
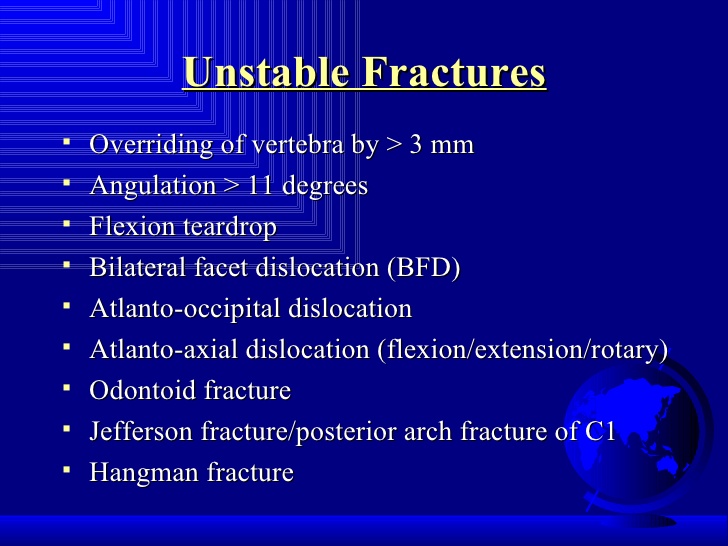
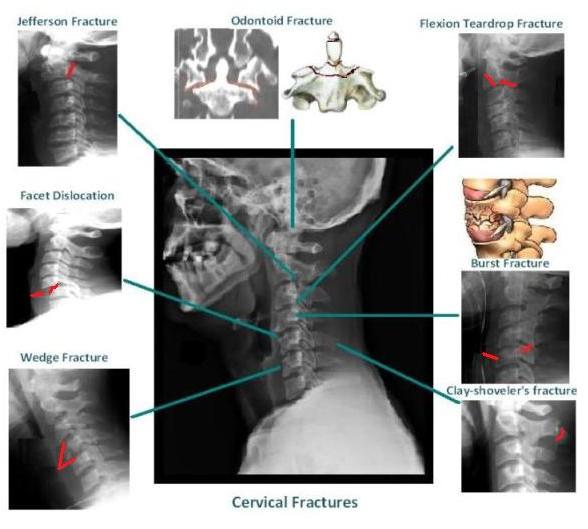
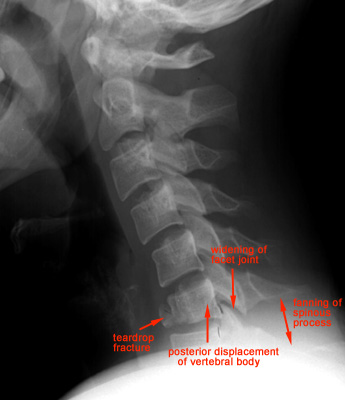
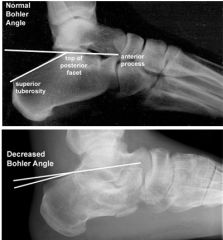
Case 1. 30yo male fell into the sand and surf while body surfing. Patient has neck pain and paralysis of extremities. Patient has decreased rectal tone and priapism. C-spine x-ray shows compression fracture of C5 with bilateral facet dislocation. Because patient had a C5 fracture and shallow respirations, he was intubated. The patient developed hypotension and bradycardia due to neurogenic shock. Neurogenic shock was treated with IV fluids and pressors. Steroids are no longer indicated for spinal cord injury. The patient was kept in C-spine immobilization. Neurosurgery was consulted.

C5 Fracture and likely bilateral facet dislocation
Case 2. 12 yo male with left hand pain after having a stingray barb impaled into the dorsum of the left hand. X-rays show no bony involvement. Hot water therapy was initiated which greatly relieved pain. The toxin of a stingray barb is exquisitely heat sensitive. Hot water will significantly diminish pain. The barb was then removed with trimming the end off and traction.

*Stingray Barb
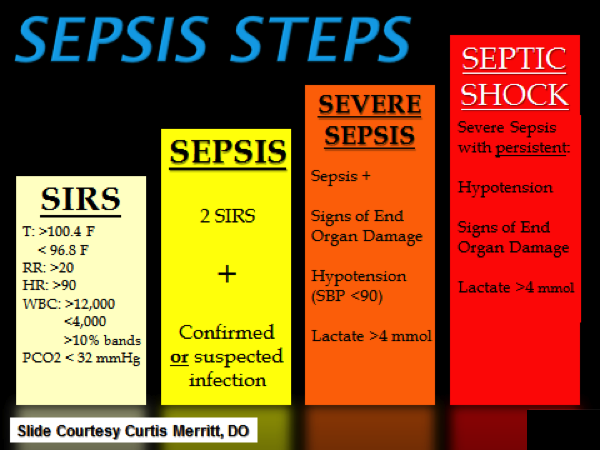
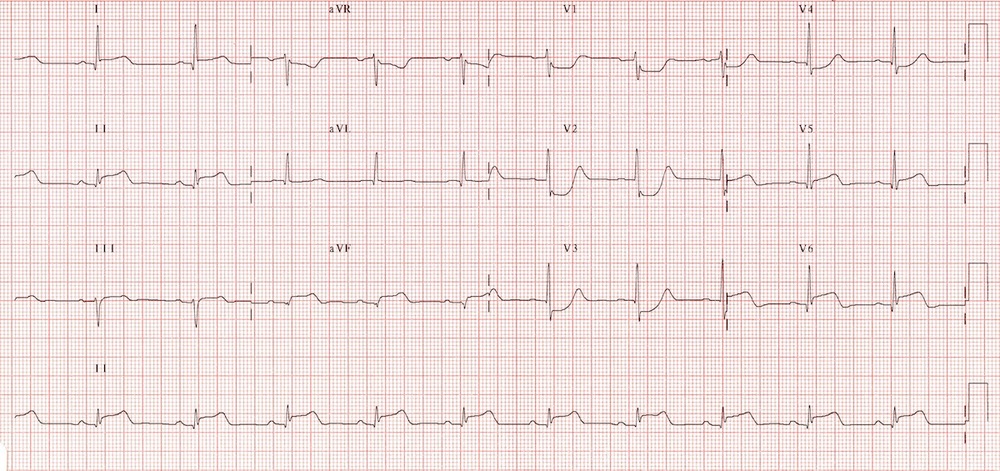
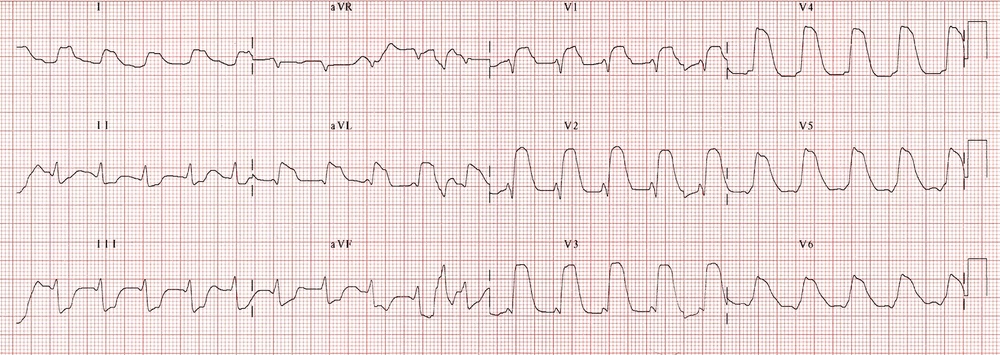
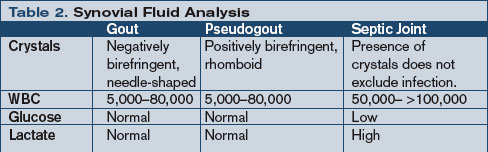
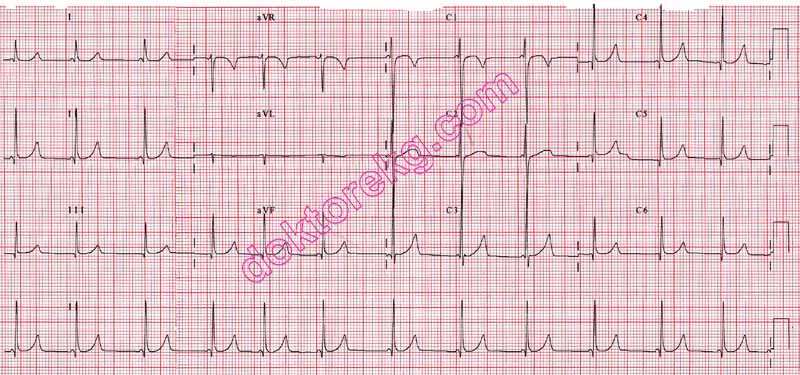
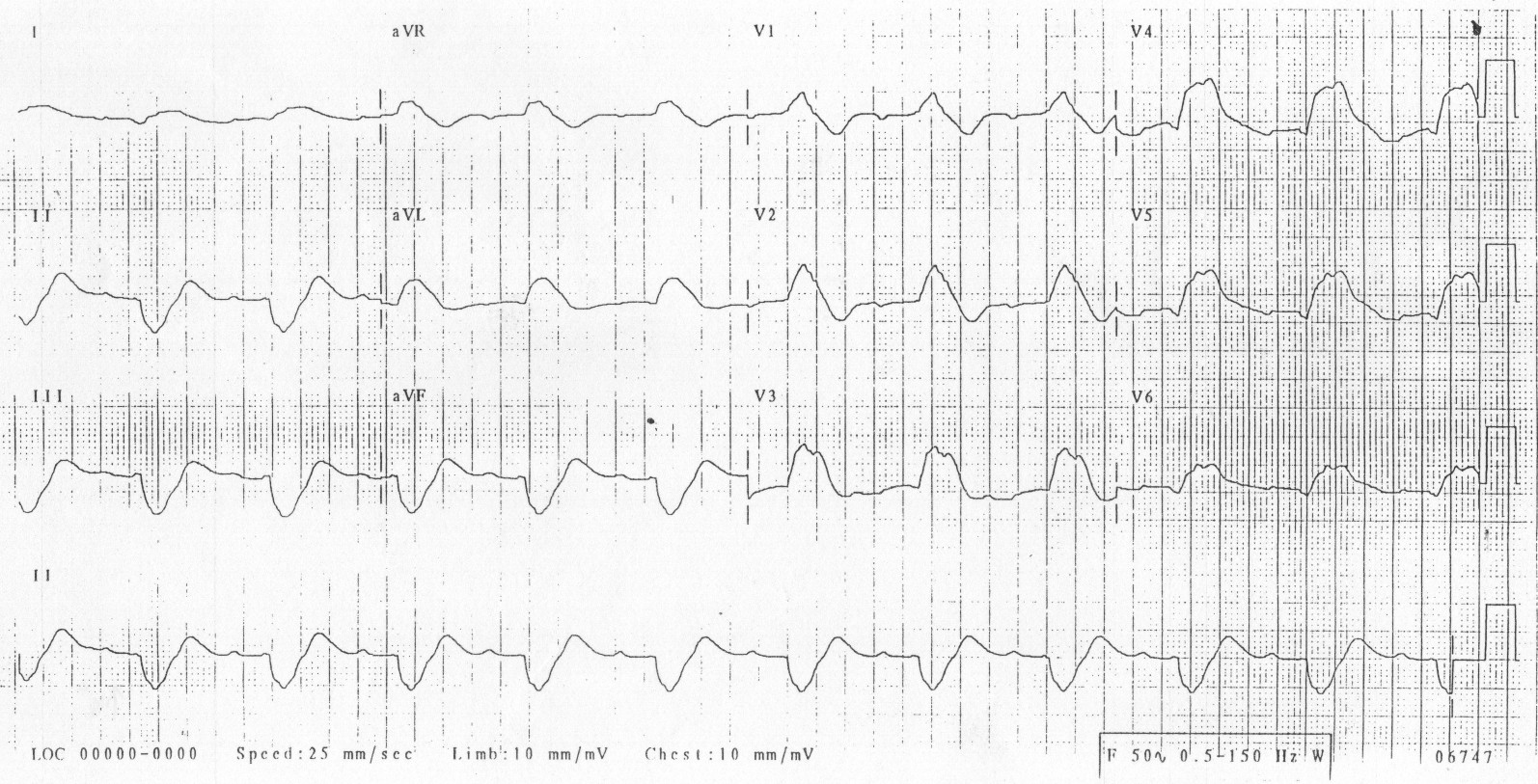
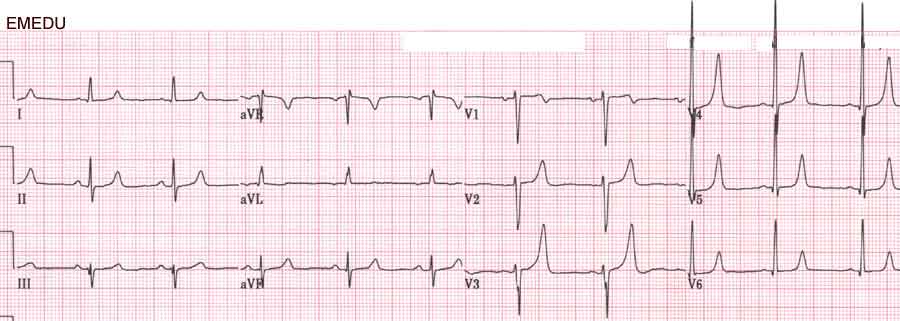
Case 3. 22yo female passed out on the beach. Temp=41.5C, HR=136. The patient had been playing volleyball and running on the beach in hot weather. On exam, patient was confused and lethargic. Skin is warm and dry. (Three keys to heat stroke diagnosis: Temp >41, dry skin, mental status changes) Rapid cooling was initiated. Goal of cooling is 39C. CPK was 9000 indicating rhabdomyolysis. Aggressive hydration was initiated to treat rhabdomyolysis. Avoid antipyretics in heat stroke because both liver and kidney are considered injured and may be very sensitive to acetaminophen and ibuprofen.
Elise comments: A pulmonary function assessment (NIF) can be useful to assess respiratory strength in a c-spine injured patients.
Look for any source of hemorrhagic shock in a trauma patient before you attribute hypotension to neurogenic shock.
Treat slimy beach envenomation’s (jelly fish) with vinegar. Treat sharp/pointy envenomation’s (stingray barbs) with hot water. It’s actually not that simple but for test taking purposes it is pretty good rule of thumb.
Chan Study Guide Genitourinary Emergencies

2015 CDC Chlamydia Treatment Guidelines

2015 CDC Gonorrhea Treatment Guidelines
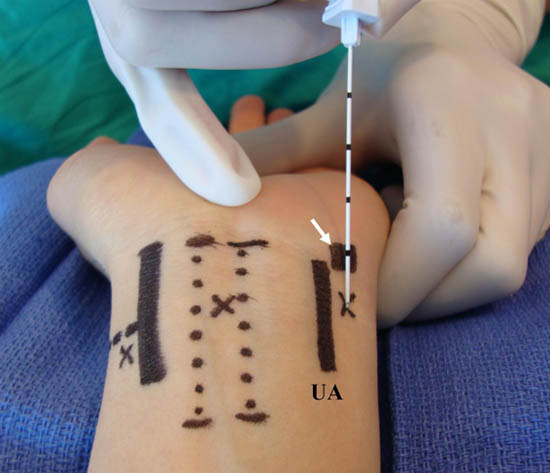
Before placing a foley in a patient with suspected urethral trauma, perform a retrograde urethrogram if you see blood at the meatus, a scrotal hematoma, or high riding prostate. If you see none of these signs, gently try to place a foley. If a foley is placed successfully, it acts as a stent for the injury and should remain in place.
Pregnant women with asymptomatic bacteruria should be treated. Asymptomatic bacteruria increases a pregnant woman’s risk of pyelonephritis. Pregnant women with bacterial vaginosis either symptomatic or asymptomatic should be treated.
Testicular torsion has 96% salvagability in the first 6 hours.
Detorsion attempts should turn the affected teste medial to lateral (opening the book). Get the patient to surgery within 6 hours from onset of pain.

Opening the Book. Medial to lateral detorsion attempt
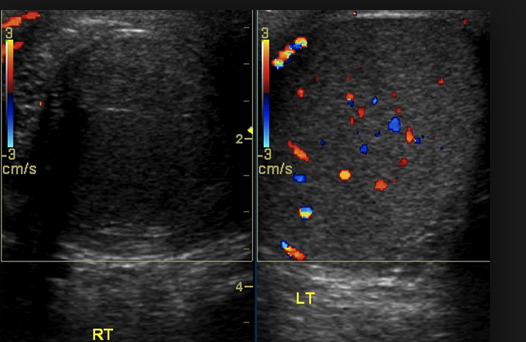
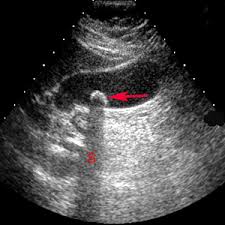
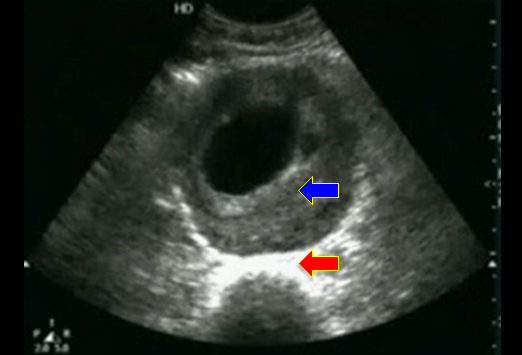
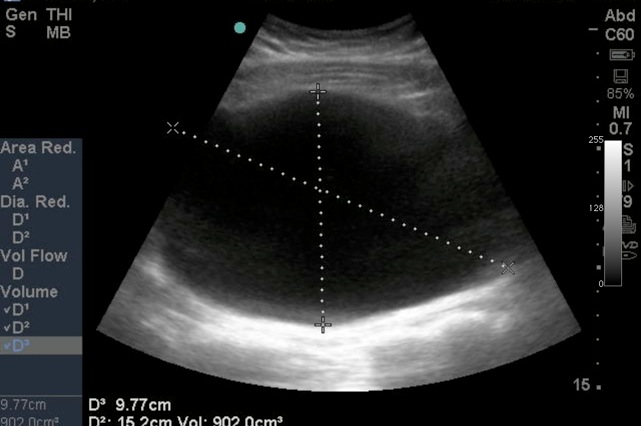
*Ultrasound of torsed teste on right. Left teste has normal flow.
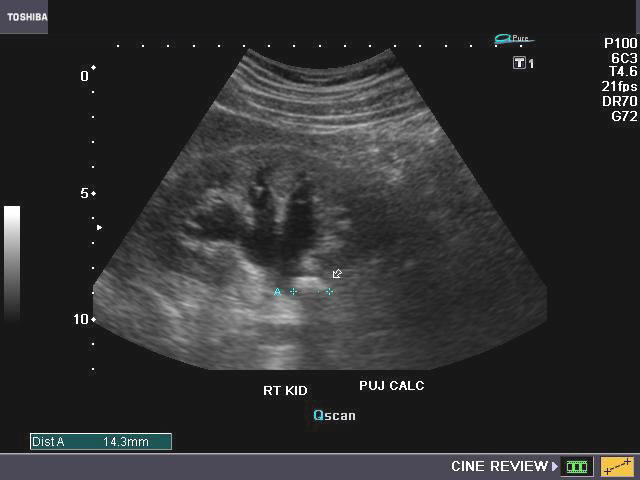
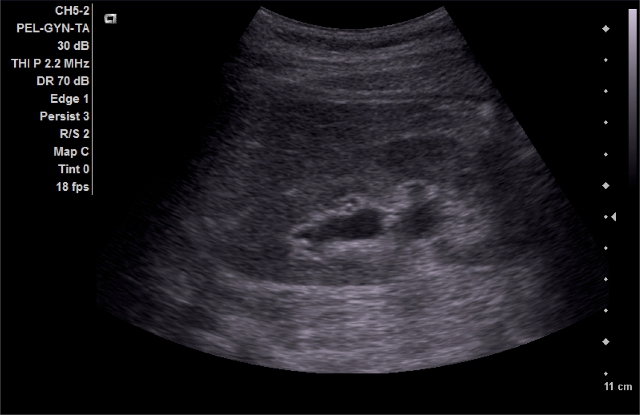
90% of kidney stones smaller than 5mm will pass within 4 weeks.

5. *Kidney stones most commonly get lodged at these 3 locations: Ureteropelvic junction, mid-ureter at pelvic brim, and at the ureterovesicular junction.
Elise comment: There are some downsides to Flomax in the elderly. It can cause postural hypotension. The newest interpretation of the data is that Flomax is most helpful in larger, upper tract stones. Flomax is less efficacious for small stones far down in the ureter.
Andrej Reference:
Quote from EM:RAP summary: December 2014:
Vincendeau, S et al. Tamsulosin hydrochloride vs placebo for management of distal ureteral stones: a multicentric, randomized, double-blind trial. Arch Intern Med. 2010 Dec 13;170(22):2021-7. PMID: 21149761.
This is probably the best study available: multicenter placebo controlled, randomized and double-blinded. They found no difference in expulsion rate (77% versus 71%) and no difference in the days to expulsion. They concluded that there was no benefit for small distal stones less than 7mm.

6. *Phimosis vs Paraphimosis Para=Around, so a paraphimosis means the foreskin is retracted around the penile shaft. Paraphimosis needs to be reduced emergently. Options include: manual compression and reduction, osmotic agents, traction with forceps, puncture techniques, and dorsal slit procedure.
Parker M&M
Case left out to protect confidential information. Take home lessons will be discussed.
If a central line is in a questionable location on CXR, you can use the “bubble test” to verify that the line is in a vessel that communicates with the RA. To do this you rapidly inject saline while visualizing the RV on ultrasound. If the line communicates with the RA, you will see turbulence in the RA with rapid injection of saline into the line.

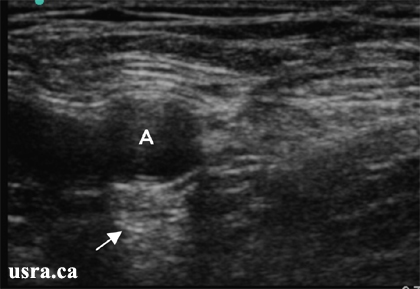
7. *US of RA showing turbulence in the RA with rapid injection of 10 ml of saline.
You can also use ultrasound to visualize the guide wire in the IJ, RA, or RV prior to dilating your access tract. To improve your visualization of the wire, use your finger to compress the vessel near the US probe. You should be able to see the wire move on US.
Elise comment: In all lines no matter how well they went, for patient safety, I recommend visualizing the wire in the IJ with ultrasound prior to dilating the vessel.
Braden also discussed a technique of placing the angiocath in the central line kit over the wire without dilating the tract. Then hooking up plain IV tubing or the wire holder in the central line kit to the angio cath to see if blood tracks up the tubing more than a few centimeters. If it does you likely have entered an artery.
You can use an ABG to detect the location of your line. You need to draw an ABG from both the line and the radial artery and compare them. This method can be problematic if you inconclusive results or you get some venous blood on the radial stick.
If you do inadvertently place a catheter in the carotid artery, don’t pull it out. Call vascular for their consultation. Pulling the line without surgical control can cause large hematomas, CNS events, and airway issues.
If you puncture the carotid artery with the needle but don’t dilate or place a catheter in the vessel, you can just pull out the needle and hold pressure for 15 minutes. Needle puncture of the carotid is less problematic than dilating and canulating the vessel.
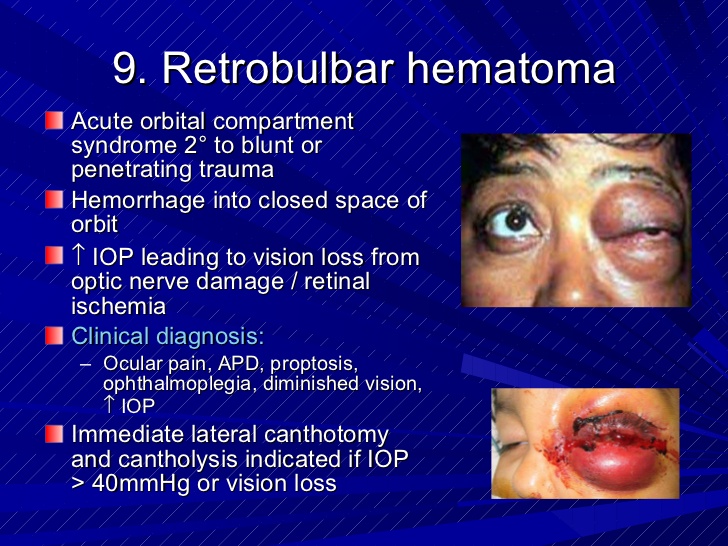
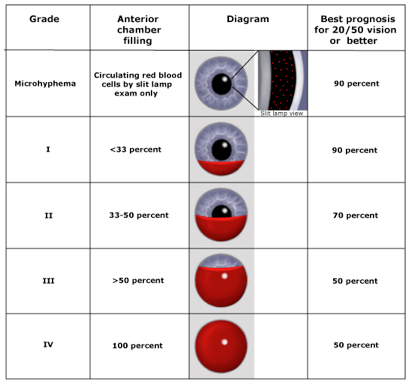
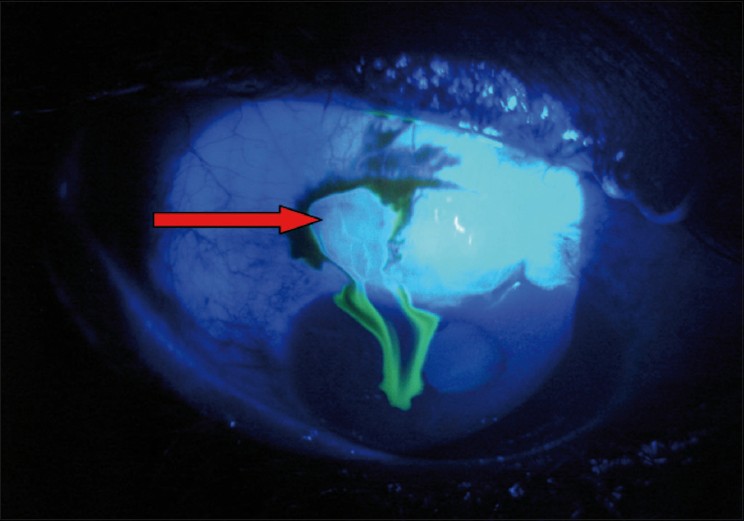
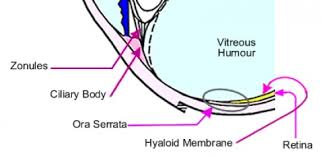
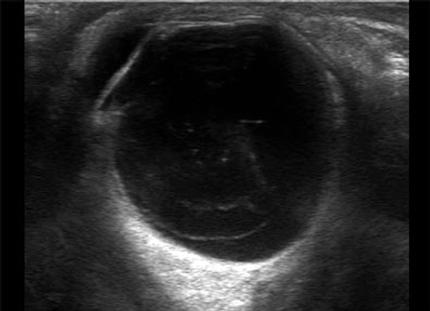
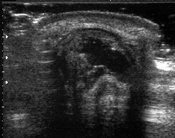
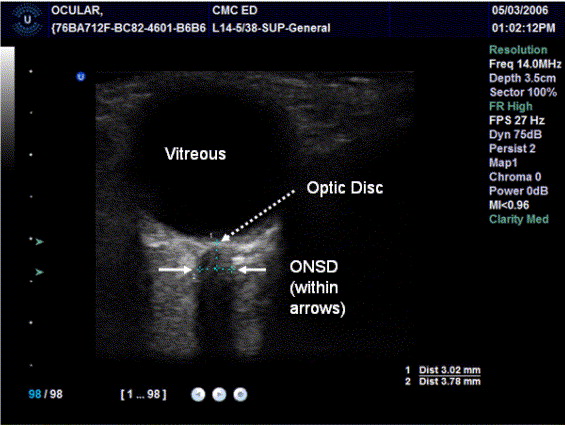
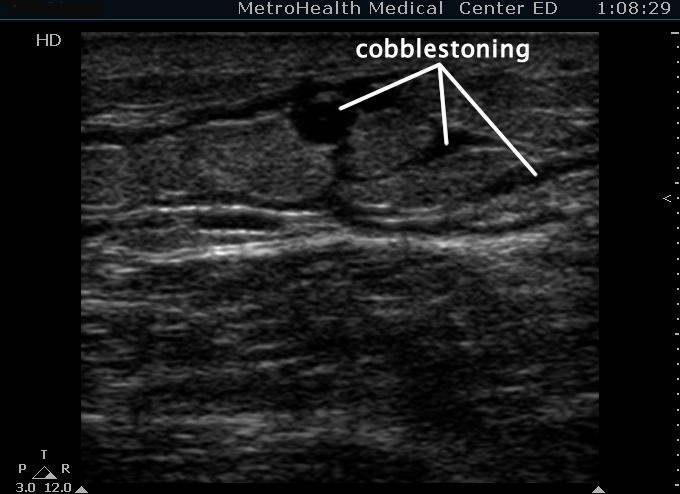
Ophthalmology Lab
Thank you to the Chiefs and Faculty for this outstanding workshop!